
CHIPRA Mandated Evaluation of the Children's Health Insurance Program: Final Findings
Download
Associated Project
CHIPRA 10-State Evaluation
Prepared for:
U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation
Key Findings
-
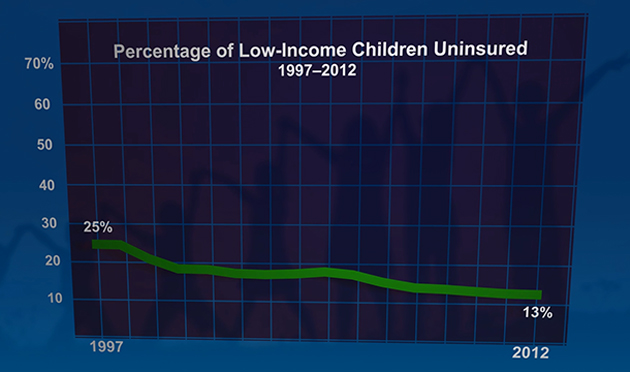
CHIP contributed greatly to the decline in uninsured rates among low-income children, which decreased from 25 percent in 1997 to 13 percent in 2012. Since CHIP was enacted, coverage rates improved for all ethnic and income groups and coverage disparities narrowed significantly for Hispanic children.
-
Relatively few low-income children in CHIP have access to private insurance coverage, and direct substitution of private for public coverage at the time of CHIP enrollment was estimated to be as low as 4 percent. Even when dependent coverage is available to families with children enrolled in CHIP, affordability is likely an important barrier many parents face in accessing employer-sponsored insurance coverage for their children.
-
Medicaid and CHIP programs worked as intended to provide an insurance safety net for low-income children, especially during times of economic hardship. Many children moved between Medicaid and CHIP; although most transitioned seamlessly, coverage gaps occurred for as many as 44 percent depending on the type of transition.
- Children in Medicaid and CHIP experienced better access to care, fewer unmet needs, and greater financial protection than children who were uninsured. Compared to children with private insurance, CHIP enrollees had better access to dental benefits and their families experienced much lower financial burden and stress in meeting the child’s health care needs. However, CHIP enrollees were less likely than children with private insurance to have a regular source of medical care and nighttime or weekend access to a provider at that source of care.
The evaluation found CHIP to be successful in nearly every area examined. CHIP succeeded in expanding health insurance coverage to the population it is intended to serve, particularly children who would otherwise be uninsured, increasing their access to needed health care, and reducing the financial burdens and stress on families associated with meeting children’s health care needs. These positive impacts were found for children and families in states with different CHIP structures and features, across demographic and socioeconomic groups, and for children with different health needs. Medicaid and CHIP have worked as intended to provide an insurance safety net for low-income children during times of economic hardship. Awareness of both Medicaid and CHIP was high among low-income families, most newly enrolling families found the application process at least somewhat easy, and the vast majority of children remained enrolled through the annual renewal period.
The evaluation also identified a few areas where there is room for improvement. One in four children in CHIP had some type of unmet need, and although most CHIP enrollees received annual well-child checkups, fewer than half received key preventive services such as immunizations and health screenings during those visits, and fewer than 40 percent had after-hours access to a usual source of care provider. Although most CHIP enrollees received annual dental checkups, a significant share did not get recommended follow-up dental treatment. There is also room for improvement in reducing the percentage of children who cycle off and back on to Medicaid and CHIP, and reducing gaps in coverage associated with moving between Medicaid and separate CHIP programs. And although participation rates have grown to high levels in most states, further effort could be targeted to the 3.7 million children who are eligible for Medicaid or CHIP but remain uninsured.
More like this from Mathematica

How do you apply evidence?
Take our quick four-question survey to help us curate evidence and insights that serve you.
Take our survey